MX-7711-02
Anesthesia machine operators should change the absorber when the absorption material changes
from white to pink/violet as the measured inspired CO
2
increases (indicating no more CO
2
can be
absorbed). The activation of an inspiratory CO
2
-high alarm limit helps to directly inform the user
about undesired levels of inspiratory CO
2
(FiCO
2
).
Another very important aspect of using rebreathing is that due to patient oxygen consumption and
dilution effects within the circle system, the inspired O
2
-level might differ to that of the set O
2
concentration in the fresh gas delivered from the system. Make sure to continuously
monitor inspired and expired values of O
2
, (FiO
2
, EtO
2
) and CO
2
(FiCO
2
and EtCO
2
).
Should the FiO
2
decrease below 21% the Flow anesthesia system has a built in safety feature,
O
2
Guard, that will automatically set the O
2
setting to 60% and, if set lower, raise the fresh gas flow
to 1 l/min. Please see the User Manual for further information.
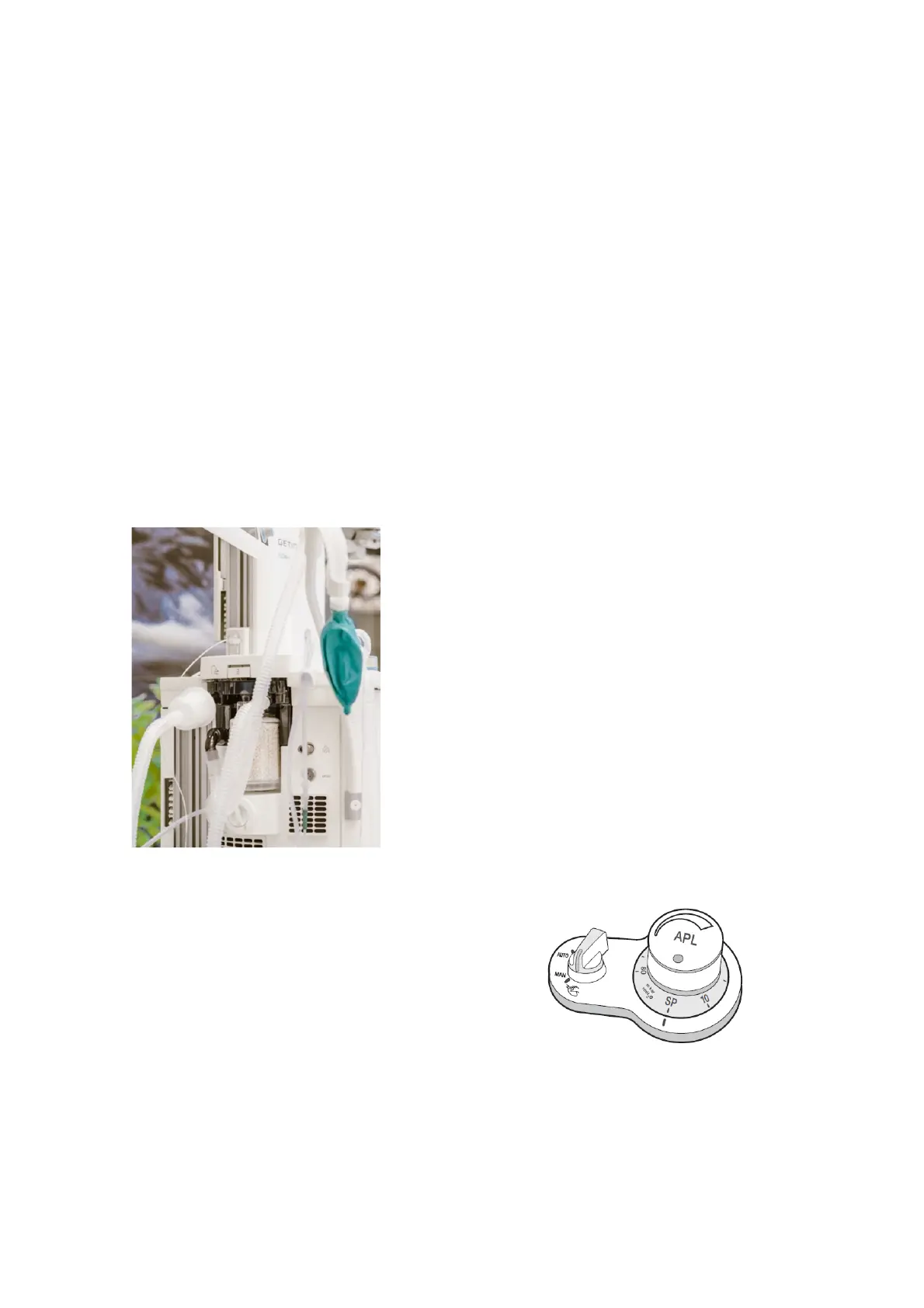
Manual and automatic ventilation (MAN/AUTO) - APL
Manual ventilation is carried out using a traditional breathing
bag connected to the patient cassette through a breathing
bag tube. During manual ventilation the ventilator is passive
which means that the patient is not ventilated unless the
manual bag is pressed and the APL is set accordingly.
The MAN/AUTO ventilation switch is an electrical switch
used to select manual or automatic ventilation. The APL
(adjustable pressure limit) valve relieves the patient circuit of
excess pressure at user defined values and ventilates the
gas into the Anesthetic Gas Scavenging System (AGSS).
When the MAN/AUTO switch is set to “MAN” the manual
ventilation valve opens and the manual ventilation bag is
connected to the breathing system.

 Loading...
Loading...




