D-0120588-B – 2019/03
Eclipse – Instructions for Use - EN Page 54
3.12 Making a ALR recording / cortical ERA
ALR/ACR threshold testing is traditionally used to help determine the degree of hearing loss in adult
populations. Compared to traditional ABR octave wide stimuli, the stimuli of ALR/ACR are much more
frequency specific due to the longer tonal and is much closer to the behavioral audiometric pure tone stimuli.
The arousal state/Patient attention of the patient has a significant effect on the amplitudes of the ALR response.
The ALR waveforms changes as a person becomes drowsy or falls asleep. When patient is asleep the N1
amplitude is smaller and the P2 amplitude is larger. However, when the subject is listening for a change or
paying close attention to stimuli the N1 increases up to 50% while P2 appears to diminish with increased
attention by the subject on the signals. The response habituates so it is important to limit the test session and
re-book if necessary.
The patient is instructed to sit quietly, alert and reading a page. It is not advised to perform ALR and P300 under
sedation (Crowley & Colrain, 2004).
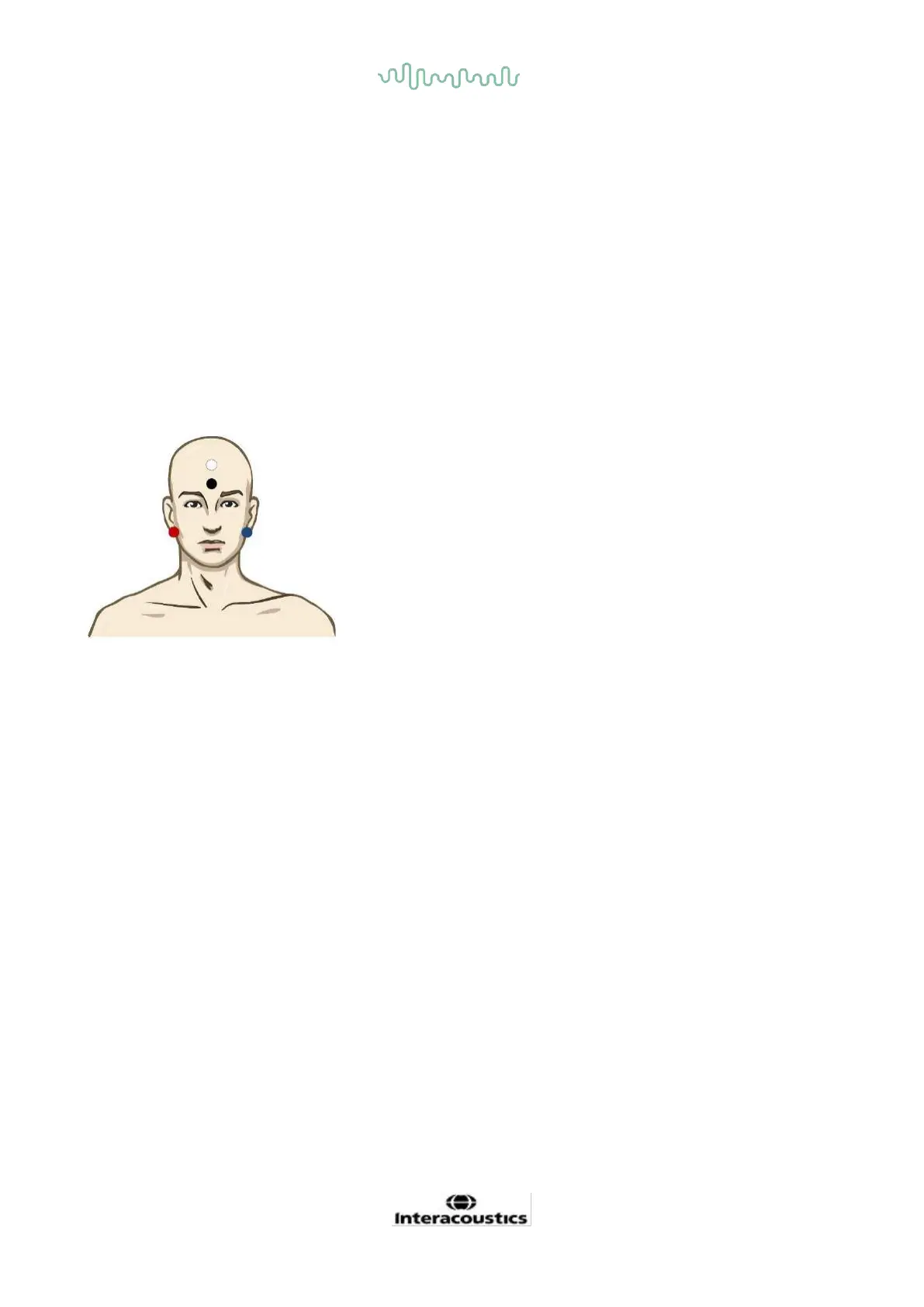
3.12.1 Example of electrode montage for an ALR threshold recording
RED Right mastoid or ear lobe (reference or inverting)
BLUE Left mastoid or earlobe (reference or inverting)
WHITE Vertex or high forehead (active or non-inverting)
BLACK Ground at cheek or low forehead - distance of few cm to WHITE electrode must be observed.
3.12.2 Stimuli
Typically the ALR threshold recording is started at 60dB nHL and decision is made to increase or lower the
stimulus intensity.
Available ALR threshold stimuli are:
• Tone bursts 250Hz – 4kHz
• Click
• Custom WAV file (when Research Module license is enabled)
 Loading...
Loading...